Infants have airways that are proportionately narrower and more susceptible to oedema than adults.
The effect of oedema can be seen in Poiseuille’s law, which states that the resistance through a tube is inversely proportional to the cube of the radius. Therefore, a small decrease in airway radius has a dramatic increase in resistance to flow.

R = resistance; l = length, v = visvocity, r = radius
Relationship between the head and neck
The infant’s head is large in relation to the rest of their body. Since the occiput is protuberant, the head tends to flex when the infant is placed supine. The larynx is also quite susceptible to external pressure at a young age. These factors combine and can result in airway obstruction when the conscious level is reduced and the child is supine.
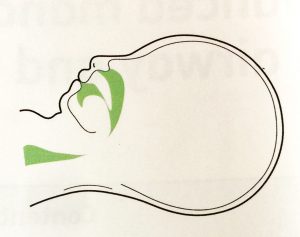
Face and mouth
Sizing of facemasks must be accurate to achieve an effective seal. The tongue is relatively large in the mouth, and the floor of the mouth is easily compressible. Care must be taken during airway manoeuvres to avoid compression of these soft tissues to prevent airway obstruction.
Beware that pressure to the eyes can result in a reflex bradycardia.
Nose and pharynx
Infants are preferential nose breathers for the first 6 months of life. Anything causing nasal obstruction can lead to increased work of breathing and respiratory compromise.
The epiglottis is large and floppy and vulnerable to iatrogenic damage
The larynx
The larynx is higher in the infant compared to the older child and adult. Until ~8 years of age, the larynx is funnel-shaped, with its narrowest segment at the level of the cricoid cartilage.
Due to the high position of the larynx, there is a sharper angle between the oropharynx and the glottis. Laryngoscopy can be challenging and a straight blade may obtain a better view than a curved blade, particularly in infants <3mo.
Airway obstruction
Recognition
Look, listen and feel.
Look for see-saw respiration, accessory muscle usage, intercostal recession.
Listen for breathing. partial obstruction will be noisy, complete obstruction silent.
Feel for air movement at the mouth and nose.
Techniques to optimise the airway
In conscious children, they will generally assume a position naturally to optimise their airway.
Unconscious children may require basic manoeuvres:
Head tilt chin lift